

How To Manage Challenging Behaviour In A Care Setting
Extract
The term 'challenging behaviour' was introduced in North America in the 1980s, and was originally used to describe problematic behaviours in people with 'mental retardation' (learning disabilities). Challenging behaviour tin, however, occur beyond the intellectual spectrum, being peculiarly prevalent in populations with psychiatric disorder.
The term 'challenging behaviour' was introduced in N America in the 1980s, and was originally used to describe problematic behaviours in people with 'mental retardation' (learning disabilities). Challenging behaviour tin, nevertheless, occur across the intellectual spectrum, being specially prevalent in populations with psychiatric disorder.
A widely accepted definition of challenging behaviour is:
"culturally abnormal behaviour of such an intensity, frequency or duration that the physical safety of the person or others is likely to be placed in serious jeopardy, or behaviour which is likely to seriously limit utilise of, or result in the person existence denied access to, ordinary customs facilities" (Reference EmersonEmerson, 1995).
Previously used terms included 'behavioural disturbance', 'problem behaviour', 'maladaptive behaviour', 'aberrant behaviour' and 'behavioural abnormalities'.
The relationship between psychiatric diagnoses and challenging behaviour is a complex i and is represented graphically in Fig. 1. Challenging behaviour tin can occur in the absence of a psychiatric disorder and not all people with mental illness exhibit challenging behaviour. The overlapping area between i and 2 represents patients with challenging behaviour and psychiatric disorder. In some people, challenging behaviour may exist an essential diagnostic criterion (e.chiliad. eating disorders, personality disorders, paraphilias, etc.) or a secondary feature (due east.grand. self-injury in depression, aggression secondary to persecutory delusions in schizophrenia and wandering in dementia). Of form, challenging behaviour may simply coexist and often pre-engagement a psychiatric disorder (e.1000. a violent offender who subsequently develops a depressive affliction). Learning disabilities and autistic spectrum disorder may also be nowadays in various combinations of comorbidity. The overlap between 1 and four represents those with dual diagnosis (mental illness and learning disabilities).
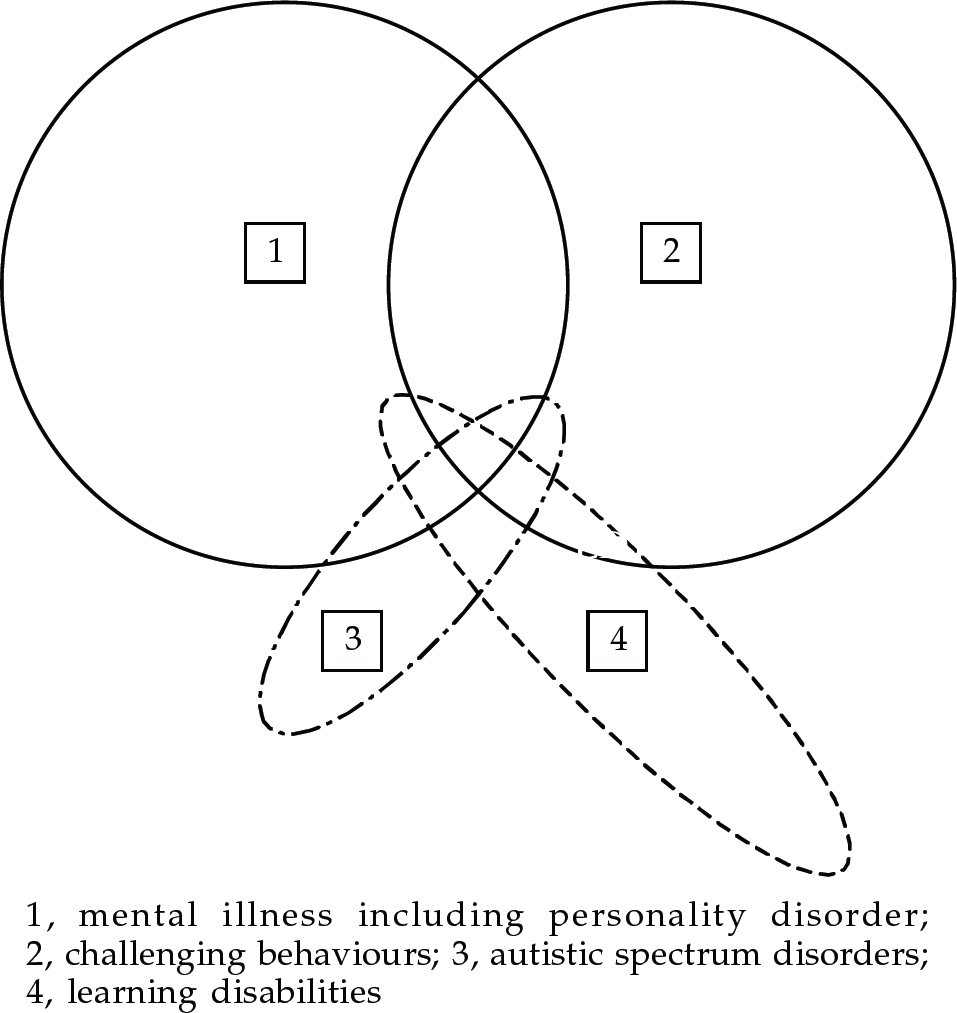
Fig. ane The relationship between psychiatric diagnosis and challenging behaviour
The part of 3 that lies outside 4 represents people with high functioning autism and Asperger'southward syndrome who may or may not have mental affliction and/or challenging behaviour.
Epidemiology
The prevalence of challenging behaviour has been near extensively studied in learning disability populations, reflecting the longer established use of the term in this field. Prevalence studies of challenging behaviour in people with learning disability vary widely in their findings, reporting rates between 5.seven% (Reference Qureshi and AlborzQureshi & Alborz, 1992) and 14% (Reference Borthwick-Duffy, Thompson and GrayBorthwick-Duffy, 1994). This probably reflects the different criteria used for case identification (for both learning inability and challenging behaviour) and the differences in the target populations (hospital and day centre communities). None the less, there is consensus that: males are more likely to be identified as having challenging behaviour than females; the overall prevalence increases with age during childhood, reaches a pinnacle during the age range xv–34 years, and and so declines; and the prevalence of challenging behaviours such as aggression and self-injurious behaviour (SIB) is greater in people with more severe learning disability (for a review see Emerson, 1995).
In the full general developed mental wellness literature, epidemiological studies of challenging behaviour every bit a single clinical entity are scarce, owing to the greater heterogeneity of clinical conditions subsumed under the title challenging behaviour (Box 1). There are, however, studies examining prevalence rates of specific trouble behaviours in adult mental health settings. For instance, Steinart et al (1999), in a study investigating the prevalence of ambitious behaviour in acute in-patient settings, found that 75% of the men in the sample and 53% of the women exhibited some blazon of aggressive behaviour (including impairment to cocky) during their beginning or subsequent access. A large number of studies have focused on the prevalence of substance misuse in clinical populations, commenting on its particular challenge for services. Regier et al (1993) established a prevalence of 29% for comorbid addictive disorders. More contempo studies have established higher rates of substance misuse among patients with severe mental disorder, with 36.3% of patients having comorbid substance misuse, which is associated with greater apply of in-patient services (Reference Menezes, Johnson and ThornicroftMenezes et al, 1996). This is of importance because comorbid substance misuse is associated with an increased prevalence of tearing behaviour and criminal offending in people with mental health bug.
Box one. Definition of challenging behaviour
Challenging behaviour is a descriptive concept, which is largely socially constructed, and its pregnant is subject area to changes in social norms and service delivery patterns over fourth dimension and across geographical areas
The term itself carries no diagnostic significance, and makes no inferences about the aetiology of the behaviour
Information technology covers a heterogeneous group of behavioural phenomena across different groups of people; for example, oppositional behaviour in children, faecal smearing in those with a severe learning disability and deliberate self-harm in adult mental illness
Challenging behaviour may exist unrelated to psychiatric disorder, but can also be a principal or secondary manifestation of it
Aetiology
Management of challenging behaviour should follow an aetiological rationale whenever possible. As challenging behaviour is not a unitary nosological entity, no single common cause for it can be identified. For instance, the aetiology of self-injury or violence is most likely different from that of disorders of sexual behaviour. Moreover, for each individual behaviour, the causation is almost invariably multi-factorial. Thus, the causes of challenging behaviour are best studied using a bio-psychosocial model to examine the different influences on the development and maintenance of challenging behaviour.
Biological factors
Genetic studies
The determinants of some challenging behaviours volition most likely closely reflect the genetics of the underlying disorder (east.one thousand. vomiting in bulimia), and in others will reflect both genetic and epigenetic factors (e.grand. violent behaviour in people with alcohol dependence or psychosis). Also, a number of genetic syndromes have been identified that are associated with varying degrees of specific maladaptive behaviour. Examples include Prader-Willi syndrome (compulsive over-eating) and Lesh-Nyhan syndrome (SIB). It has been proposed that study of these disorders may allow further agreement of the genetic contribution to detail behaviours. To this stop, the concept of behavioural phenotypes has been introduced to describe the behavioural manifestations of a particular genetic make-upwards (genotype). However, at that place are a number of methodological problems in the study of behavioural phenotypes - including lack of appropriate instruments, the subjective nature of behavioural observations and difficulty in identifying a behavioural standard. None the less, the report of some groups of people with genetically determined syndromes does allow a more than fine-grained analysis of the genetic and epigenetic contributions to challenging behaviours in that group of people, and may also allow usa to further empathize the biological basis to psychiatric disorder in the general population. For example, people with velo-cardio-facial syndrome (VCFS) take a deletion at Q11 on chromosome 22 (the catechol-O-methyl transferase gene is in this region) and upwards to 30% of people with VCFS take psychosis.
Neurochemical studies
A number of endogenous substances have been investigated for their role in the development and maintenance of challenging behaviour. In detail, opioid peptides (β-endorphins), sexual activity hormones, dopamine and serotonin have been studied in relation to their role in mediating human behavioural processes such as aggression, arousal, self-injury and appetite. Endogenous opioids have been implicated in the pathophysiology of SIB and a number of aetiological pathways accept been hypothesised, for example, the intrinsically rewarding properties of endorphins released past SIB. Serotonin has been implicated in SIB, aggression, stereotypies, anxiety and behavioural disinhibition. Testosterone has been implicated in the mediation of ambitious and abnormal sexual behaviour. In item, impulsive aggression in personality disorder correlates with tritiated paroxetine binding in the platelet. All the above-mentioned aetiological pathways have been utilised as the neurochemical ground of pharmacotherapeutic interventions.
Brain structure and office
The relationship betwixt item abnormalities in brain structure and function and well-defined challenging behaviours is poorly researched (for an overview, encounter Robertson & Murphy, 1999). Thus, although at that place are many studies on neurobiological differences between people with psychiatric disorder and controls, there are relatively few which have related the frequency and severity of individual challenging behaviours to particular biological variables. None the less, some progress has recently been fabricated, for example, in agreement the neurobiological correlates of vehement behaviour. Lesion studies have implicated a number of brain areas in the regulation of aggression, including the amygdala-hippocampal circuitous and prefrontal cortex (Reference Mirsky and SiegelMirsky & Siegel, 1994). Qualitative computerised axial tomography (CT) and quantitative positron emission tomography (PET) studies accept reported anatomical abnormalities, and reduced glucose metabolism, in prefrontal and temporal regions. Nevertheless, until recently, nobody had related neurobiological variables to frequency of violence, or used quantitative in vivo techniques to investigate neuronal integrity and brain anatomy of people who are repetitively violent. Thus, we used proton magnetic resonance spectroscopy (HMRS) to study the neuronal integrity of the prefrontal lobe and amygdala-hippocampal complex in repetitively violent adults and not-violent matched controls. We constitute that repetitively vehement people had reduced neuronal density and aberrant phosphate metabolism in the prefrontal lobe and amygdala-hippocampal complex, and the degree of reduced neuronal density was related to frequency of violence (Reference Critchley, Simmons and DalyCritchley et al, 2000).
Psychosocial factors
A wide range of theoretical frameworks present conceptualisations of challenging behaviour, including psychoanalytic and sociological theories. Even so, clinical approaches derived from learning theory, which have been subject to the rigours of empirical validation, will exist the main focus of this paper.
The functionalist approach
The majority of inquiry into psychological factors underpinning the aetiology of challenging behaviour has taken a functional perspective, with its origins in learning theory. In this approach, the accent is on the purpose the behaviour serves for the individual, rather than the grade of the behaviour per se. Alternative hypotheses relating to the functions of the target behaviour are developed (functional assessment) and can be evaluated systematically (functional analysis). In addition to accessing or avoiding either external or internal events, challenging behaviour may as well serve as a grade of communication. A unmarried challenging behaviour tin can also exist multi-functional (for a review encounter Sturmey, 1996) and there is an emphasis on internal events and emotion in the modern functional analysis.
Experimental research on challenging behaviours has, once more, historically focused on people with learning disability, seeking to evaluate cess and handling procedures. For example, a large number of studies have investigated SIB, terminal that information technology is oftentimes a learned behaviour, acquired through an individual'south history of interaction with his or her social and/or physical environment. Studies which have applied the methodology of functional analysis to large numbers of cases conclude it to be highly effective in identifying the environmental determinants of SIB on an private basis (Reference Iawata, Pace and DorseyIawata et al, 1994). Moreover, treatments are only effective when they match the functions of the target behaviour appropriately.
More than recently, the methodology of functional analysis has been applied in populations without learning disability, for example, in conditions as diverse every bit anorexia nervosa, delusional speech and hallucinatory behaviour, problem-drinking and personality disorder.
Assessment and treatment of challenging behaviour
Service delivery issues
Challenging behaviours do non e'er come up to the attention of health intendance professionals. A big proportion of people who exhibit challenging behaviour are dealt with by the penal system (east.g. prison house rehabilitation or probation service), the educational system (e.g. educational psychologists or special schooling), or social services and the voluntary sector (east.g. supported housing, twenty-four hours and respite care provision). Specifically in the population with learning disability, challenging behaviour can be a significant obstacle to resettlement in the community and a frequent cause of requests for admission or re-access to infirmary (Reference Mansell and BourasMansell, 1994). Currently, the National Health Service spends over £600 million on services for people with learning inability. In improver, local regime spend approximately £400 million (Inspect Commission, 1992). Information technology is not known what proportion of this expenditure is spent on challenging behaviour services, but given the loftier prevalence of challenging behaviour in learning inability, with services needing to be highly resourced, it is likely to be a meaning amount. When people with challenging behaviour, with or without learning disability, do receive wellness care, it is usually within the mental health care system - just the detail service model varies in location and treatment methods employed. Thus, services may be delivered by general adult psychiatric services (including community mental health teams, intensive-intendance units and challenging-behaviour units), neuropsychiatric services (including brain injury and epileptology services), learning disabilities teams, forensic psychiatric services and child and adolescent teams.
Both cess and treatment found integral components of the direction of patients with challenging behaviour, and the 2 processes may not be easily distinguishable - as continuous reassessment often merges with treatment process. Thus, the setting of the patient's direction needs to be carefully considered. Out-patient treatment is the obvious kickoff option, provided that safe issues are taken into account. It has the advantage of treating persons in their natural environment, thereby limiting the problems in generalisation of handling response from in-patient to customs settings. None the less, hospitalisation may exist indicated because of the frequency and severity of the challenging behaviour, and specialist in-patient units offer an constructive treatment pick for certain groups of people (Reference Xenitidis, Henry and RussellXenitidis et al, 1999). The employ of a legal framework nether the Mental Health Human activity (MHA) may be necessary under sure circumstances, when the patient is thought to be suffering from ane of the 4 categories of mental disorder (mental illness, psychopathic disorder, mental damage and astringent mental damage). The importance that the legislation attaches to challenging behaviour is indicated by the fact that the 3 categories defined in Section 1 of the MHA (mental illness is not divers) require a behavioural criterion ("seriously irresponsible or abnormally aggressive behaviour") to be satisfied in gild for the person to be idea of equally suffering from 1 of these disorders. For mental impairment and severe mental impairment, the behaviour needs to "exist associated with" the condition, whereas for psychopathic disorder the behaviour must be "the effect of" the condition.
The general principles for the management of challenging behaviour are shown in Box 2.
Box 2. Service issues in the management of challenging behaviour
Direction needs to be tailored to the individual person, taking into account the particular behaviour and the setting in which information technology occurs
Multi-agency, multi-disciplinary involvement is necessary, and it is essential to gather detailed information about the nature and outcome of previous interventions
Different treatment modalities, i.eastward. pharmacotherapy, psychological and social interventions, alone or in combination, may be required. Merely i treatment should exist introduced at a fourth dimension
The safety of the person displaying the challenging behaviour and of others must be considered carefully. A detailed risk assessment should be conducted, and the degree of urgency of response decided
Treatment in a safe and secure environment, if necessary within the framework of the Mental Health Act in a specialised unit of measurement, may need to be considered
General principles
Whatever the setting and the legal framework, the management of challenging behaviour is typically resources-intensive. Ofttimes, a single agency may take the atomic number 82, but collaboration between a number of agencies volition be necessary. Inside each agency, a number of disciplines will need to be involved in both the assessment and the treatment phase. The drove of groundwork information from a number of sources is essential if an accurate conception of the development of the challenging behaviour is to exist made, and the risk associated with it minimised. Detailed review of patients' medical, educational and social records is time-consuming simply necessary for clarifying the degree of success of previous formulations and interventions. Medical investigations will be required, as appropriate, into the presence of whatsoever comorbid medical status or mental disorder. If a causative clan is suspected, the management of causality should be adamant.
Information should be gathered from a diverseness of sources, including an individual's self-written report, interview with family and carers, and direct observation of behaviour. Management should be guided by the principles of sequential single hypothesis testing. That is, the challenging behaviour should be quantified at baseline, and the effectiveness of each intervention assessed by accurately, and reliably, measuring pre- and post-treatment levels (Box three). Only i treatment should be introduced at a time, and response to that treatment should be measured before it is replaced or augmented by others. In this way, the particular benefits of specific treatments can be evaluated, allowing later refinement of focused service delivery.
Box 3. Steps towards systematic cess and treatment of challenging behaviour
Identification of target behaviour(southward)
Quantitative measurement of target behaviour
Generation of hypotheses (medical, psychological and social) nearly the genesis and maintenance of the behaviour
Delivery of therapeutic intervention designed to examination the hypotheses adult in line with a sequential, single hypothesis-testing model
Evaluation of effectiveness of the intervention
Generation and testing of alternative hypotheses
The use of standardised assessment tools facilitates the reliable and accurate measurement of the target behaviour. Several scales be which provide comprehensive cess of domains of challenging behaviour, for example, the Adaptive Behaviour Scale (Reference Nihira, Foster and ShellhaasNihira et al, 1974). Nonetheless, these were primarily developed for employ with people with learning disability and do not generalise well to the general adult population. Although each clinical speciality may possess its own tailored measures to describe and categorise issues presented in that clinical area (e.g. Body Mass Index in eating disorders), people may also have a number of generic problems which require broader assessment tools (e.g. self-injury or depression). For instance, the Overt Aggression Scale (OAS) for the Objective Rating of Verbal and Physical Assailment (Yudofsky, 1986) allows verbal and concrete aggression to others, self and property to be evaluated in a clinically applicable format. Every bit noted above, the aim of this role of the assessment is to measure considerately the frequency and severity of the challenging behaviour and any putative determining factors.
Close attention must be paid to the reliability and validity of measures that are used, and the assessment should be multi-modal, rather than relying on a single source of information. Direct naturalistic observations of the behaviour, and related events, tin exist systematically recorded on A-B-C charts. Here, the antecedents (A), behaviour (B) and its consequences (C) are described and the contingent relationships analysed. Behaviour can also be recorded using a range of idiosyncratic observational schemes. The nigh commonly employed are sampling schemes, where behaviour is observed and recorded at predefined temporal intervals. Intervals can be scored according to a number of rules. Observations of behaviour via such 'samples' are represented every bit directly proportional to 'real time'. Alternatively, behaviour can exist observed via counterpart conditions, where environmental events are systematically manipulated, and the effect on behaviour observed, to decide which reinforcers are operative in the natural surround.
Whatever the methods employed, information gathered should aim to:
-
(a) establish the backdrop (frequency, duration, etc.) of the behaviour at 'baseline' point in time;
-
(b) develop and evaluate culling hypotheses relating to the functions of the behaviour;
-
(c) predict the times and situations when the behaviour will and will not be performed beyond the total range of typical daily routines;
-
(d) define the role that the behaviour serves for the private.
Specific therapeutic interventions
Pharmacotherapy
The treatment of an underlying mental disorder, epilepsy or other physical status should exist the target of any specific medication in the first instance. The full general principles of pharmacotherapy should follow the principles highlighted in the section on Aetiology.
Cocky-injury
The opioid antagonists naloxone and naltrexone take been used for the reduction of SIB in learning disability patients. It is thought that this reduction is mediated by a selective blockade of endorphin receptors leading to removal of the biologically based reinforcing properties of cocky-injury. In that location have as well been reports on the constructive use of serotonergic antidepressants for the handling of SIB.
Sexually inappropriate behaviour
Antilibidinal drugs such equally cyproterone acetate have been used with recidivist sex offenders and other patients repeatedly exhibiting unacceptable or dangerous sexual behaviour. The machinery of action of antilibidinal drugs is thought to be through a reduction of circulating androgens in the blood stream. As testosterone has been associated with aggressive as well as hypersexual behaviour, these drugs may deed on both components of complex aggressive sexual behaviour, reducing its manifestation. Although all neuroleptic drugs accept an antilibidinal effect that is usually regarded equally a side-event of their employ equally antipsychotics, benperidol is thought to have a more marked antilibidinal consequence, and sexually inappropriate behaviour is included in its formulary indications.
Aggression
Although some drugs have been marketed as having a specific anti-aggressive upshot (lithium and chlorpromazine), information technology is more likely that whatsoever reduction of aggression is either secondary to a reduction of a primary psychopathology, or results from a not-specific sedative issue (Box iv). Neuroleptics, benzodiazepines (caution is required considering of possibility of paradoxical excitement), mood stabilisers and antidepressants have all been used for the treatment of ambitious behaviour.
Box 4. Controversial issues in the management of challenging behaviour
Challenging behaviour is a socially constructed concept, and equally such represents an entity of questionable validity
There exists no consensus nigh the borders between health and social intendance and what constitutes a wellness or social outcome in relation to challenging behaviour
Interventions for challenging behaviour (including concrete restraint, seclusion/exclusion and programmes based on the principles of reinforcement) accept the potential to be misused as penalty or a method of social control
The utilize of drug handling for challenging behaviour with no clearly understood neurochemical basis, and with no testify of underlying mental illness, may be both ethically and scientifically dubious
Use of the Mental Health Act for challenging behaviour may be open to abuse
Controversy nigh the virtually appropriate clinical speciality may result in patients 'falling between two stools'
Psychological treatments
From a learning theory perspective, Goldiamond (1974) outlines two contrasting approaches to the assessment and treatment of problematic behaviours. The pathological approach views challenging behaviour as a problem that has to be suppressed or removed. Although many studies report effective suppression of targeted challenging behaviour (e.thou. by extinction), interventions based on a pathological approach can be described as 'prosthetic', and there are well-established bug with generalisation across settings, long-term maintenance and symptom substitution. The constructional approach views challenging behaviour equally a successful means of serving a part. It can be seen in an individual whose resources are compromised as a legitimate and logical path to a desired natural result, admitting pitiful to the person or others. Interventions based on a constructional approach focus on establishing new, less sad behaviours, which will serve the same office, leading to the same natural effect.
Behaviour modification
Treatment within a behaviour modification framework is based on the systematic analysis and awarding of reinforcement. Reinforcement is the procedure by which new responses are acquired and existing ones are strengthened. Information technology refers to the procedure of providing consequences for the behaviour that increase or maintain the frequency of that behaviour. A reinforcer is defined by its results. Reinforcement programmes can manipulate the schedule, ratio and nature of reinforcers. Restructuring the environs to remove significant contingent events may also be viewed as necessary; for case, social relationships associated with patterns of addictive behaviour may be avoided until the individual feels confident about renewing acquaintances without reverting to onetime patterns of behaviour.
Cess of challenging behaviour using functional assay can help to place for the individual alternative behaviours that will produce desirable consequences similar to those of the challenging behaviour. The person is and so encouraged to substitute these culling behaviours in settings that would ordinarily elicit the target behaviour. This is called solution assay and is a handling arroyo of established therapeutic value. For example, it has been demonstrated that functional and subsequent solutional analyses of parasuicidal acts result in fewer incidents of parasuicidal behaviour and fewer in-patient days than standard therapies (Reference Linehan, Heard and ArmstrongLinehan et al, 1993). The skills inherent in producing the alternative behaviour may need to exist learned/shaped, every bit they may non be present in the individual'south repertoire.
Cognitive-behavioural therapy
The cerebral model and its applied application in clinical psychology have allowed psychological interventions to become more targeted in their use of internally generated fabric as a focus for treatment. Cognitive-behavioural therapy (CBT) encompasses a broad range of interventions, offered to clients within the framework of 'collaborative empiricism'. As well as behavioural strategies for managing symptoms, thoughts, beliefs and feelings are perused and examined for relevance and validity. Traditional or 'elegant' cerebral therapy was developed to work either in combination with pharmacotherapy or lone to ameliorate the symptoms of low in adults. The success of CBT as an effective intervention has encouraged clinicians and researchers to investigate and use its techniques in a wide range of clinical problems; these include low (for a review, see Watkins & Williams, 1998), panic (Reference Clark, Salkovskis and HackmanClark et al, 1994), psychotic symptoms (Reference Garety, Kuipers and FowlerGarety et al, 1994) and personality disorder (Reference Nelson-Grayness and FarmerNelson-Gray & Farmer, 1999). More recently, the efficacy of CBT as a handling for adults with mild learning inability has been established (Reference Lindsay, Howells and PitcaithlyLindsay et al, 1993), although, to engagement, sample sizes have been modest.
Psychodynamic and systemic therapies
Individual, family unit and group psychotherapeutic approaches based on systemic or psychodynamic theories accept been used in the treatment of challenging behaviour, either alone or as an adjunct to other therapeutic modalities. Data on their effectiveness and efficacy are express, especially in the learning inability field. Although a number of case reports and review articles take been published in contempo years, peculiarly in the area of forensic psychotherapy and psychological treatments of people with personality disorders, further research on both the process and the event of psychotherapeutic approaches is needed.
Multiple choice questions
-
1. The term challenging behaviour:
-
a implies unknown aetiology
-
b is reserved for people with a learning disability
-
c cannot exist used for people with mental illness
-
d is socially constructed
-
e does not utilize to people with autism.
-
-
ii. Treatment of challenging behaviour:
-
a should avoid pharmacotherapy
-
b is nearly always multi-disciplinary
-
c an in-patient setting should be avoided
-
d should avoid the simultaneous introduction of two treatment modalities
-
e depends on underlying aetiology.
-
-
iii. Out-patient treatment of challenging behaviour:
-
a may exist too risky to undertake
-
b is well-nigh always the preferred pick
-
c should always exist used with adolescents
-
d prohibits use of psychotherapeutic techniques
-
e is never viable with offenders.
-
-
four. In the management of challenging behaviour, the Mental Health Act:
-
a should be used only if at that place is an underlying affliction
-
b is not applicable to adolescents
-
c is applicable in severe learning disability
-
d is simply applicable to offenders
-
eastward is well-nigh always ethically dubious.
-
-
5. The constructional arroyo to challenging behaviour implies:
-
a providing negative consequences for the behaviour
-
b viewing the behaviour as successfully serving a office
-
c highlighting further education
-
d aiming to replace the challenging behaviour with behaviour serving the same function
-
e defining the pattern of reinforcement.
-
MCQ answers
| 1 | 2 | 3 | 4 | 5 | |||||
|---|---|---|---|---|---|---|---|---|---|
| a | F | a | F | a | T | a | F | a | F |
| b | F | b | T | b | T | b | F | b | T |
| c | F | c | F | c | F | c | T | c | F |
| d | T | d | T | d | F | d | F | d | T |
| due east | F | e | T | e | F | e | F | e | F |
References
Audit Commission (1992) Community Care: Managing the Cascade of Intendance. London: HMSO.Google Scholar
Borthwick-Duffy, S. A. (1994) Prevalence of destructive behaviors. In Destructive Behavior in Developmental Disabilities: Diagnosis and Treatment (eds Thompson, T. & Greyness, D. B. ) pp. three–23. Thousand Oaks, CA: Sage.Google Scholar
Clark, D. One thousand. , Salkovskis, P. M. , Hackman, A. et al (1994) A comparison of cognitive therapy, applied relaxation and imipramine in the treatment of panic disorder. British Periodical of Psychiatry, 164, 759–769.CrossRefGoogle ScholarPubMed
Critchley, H. , Simmons, A. , Daly, East. et al (2000) Prefrontal and medial temporal correlates of repetitive violence to self and others. Biological Psychiatry, 47, 928–934.CrossRefGoogle ScholarPubMed
Emerson, Eastward. (1995) Challenging Behaviour. Analysis and Intervention in People with Learning Difficulties. Cambridge: Cambridge University Press.Google Scholar
Garety, P. A. , Kuipers, Due east. , Fowler, D. et al (1994) Cognitive–behavioural therapy for drug-resistant psychosis. British Journal of Medical Psychology, 67, 259–271.CrossRefGoogle ScholarPubMed
Goldiamond, I. (1974) Toward a constructional approach to social bug. Behaviourism, i, 1–84.Google Scholar
Iawata, B. A. , Step, One thousand. M. , Dorsey, M. F. et al (1994) The functions of self-injurious behaviour: an experimental epidemiological analysis. Journal of Applied Behaviour Analysis, 27, 215–240.CrossRefGoogle Scholar
Lindsay, W. R. , Howells, L. & Pitcaithly, D. (1993) Cognitive therapy for depression with individuals with intellectual disabilities. British Journal of Medical Psychology, 66, 135–141.CrossRefGoogle ScholarPubMed
Linehan, Yard. , Heard, H. & Armstrong, H. (1993) Naturalistic follow-up of a behavioural treatment for chronically parasuicidal borderline patients. Archives of General Psychiatry, 50, 971–974.CrossRefGoogle ScholarPubMed
Mansell, J. (1994) The challenge of providing high quality services. In Mental Health in Mental Retardation (ed. Bouras, N. ) pp. 328–340. Cambridge: Cambridge Academy Press.Google Scholar
Menezes, P. R. , Johnson, S. , Thornicroft, One thousand. et al (1996) Drug and alcohol problems among individuals with several mental illness in s London. British Journal of Psychiatry, 168, 612–619.CrossRefGoogle ScholarPubMed
Mirsky, A. F. & Siegel, A. (1994) The neurobiology of violence and aggression. In Understanding and Preventing Violence. Vol. Ii Biobehavioural Influences, pp. 59–172. Washington, DC: National Academic Press.Google Scholar
Nelson-Greyness, R. O. & Farmer, R. F. (1999) Behavioural cess of personality disorders. Behaviour Research and Therapy, 37, 347–368.CrossRefGoogle ScholarPubMed
Nihira, K. , Foster, R. , Shellhaas, M. et al (1974) AAMD Adaptive Behaviour Scale. Washington, DC: American Clan of Mental Deficiency.Google Scholar
Qureshi, H. & Alborz, A. (1992) Epidemiology of challenging behaviour. Mental Handicap Inquiry, 5, 130–145.CrossRefGoogle Scholar
Regier, D. A. , Narrow, W. E. , Rae, D. S. et al (1993) The de facto U.s. mental and addictive disorders service system. Epidemiologic catchment surface area prospective 1-year prevalence rates of disorders and services. Archives of General Psychiatry, 50, 85–94.CrossRefGoogle Scholar
Robertson, D. & Irish potato, D. Chiliad. M. (1999) Brain imaging and behaviour. In Psychiatric and Behavioural Disorders in Developmental Disabilities and Mental Retardation (ed. Bouras, N. ) Cambridge: Cambridge University Press.Google Scholar
Steinart, T. , Wiebe, C. & Gebhardt, R. P. (1999) Aggressive behaviour against self and others among first-admission patients with schizophrenia. Psychiatric Services, l, 85–90.CrossRefGoogle Scholar
Sturmey, P. (1996) Functional Analysis in Clinical Psychology. Chichester: John Wiley & Sons.Google Scholar
Watkins, E. & Williams, R. (1998) The efficacy of cognitive-behavioural therapy. In The Management of Depression (ed. Checkley, South. ) Oxford: Blackwell.Google Scholar
Xenitidis, G. I. , Henry, J. , Russell, A. J. et al (1999) An inpatient handling model for adults with mild intellectual disability and challenging behaviour. Journal of Intellectual Disability Enquiry, 43, 128–134.CrossRefGoogle ScholarPubMed
Yudofsky, S. C. , Silvery, J. M. , Jackson, W. et al (1986) The Overt Aggression Scale for the objective rating of verbal and concrete assailment. American Journal of Psychiatry, 143, 35–39.Google ScholarPubMed

How To Manage Challenging Behaviour In A Care Setting,
Source: https://www.cambridge.org/core/journals/advances-in-psychiatric-treatment/article/management-of-people-with-challenging-behaviour/E7EF8F63420EEB53CC34EEB217100B31
Posted by: harrisfropmed.blogspot.com
0 Response to "How To Manage Challenging Behaviour In A Care Setting"
Post a Comment